Mastering Diabetes Insipidus and SIADH in Preparation for NCLEX Exam
Diabetes insipidus (DI) and Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) are critical topics for the NCLEX exam, as they involve key concepts related to fluid and electrolyte balance. Understanding the pathophysiology, symptoms, diagnosis, and management of these conditions is essential for providing effective nursing care. This blog post provides a comprehensive guide to help you prepare for the NCLEX exam.
Diabetes Insipidus (DI)
Pathophysiology
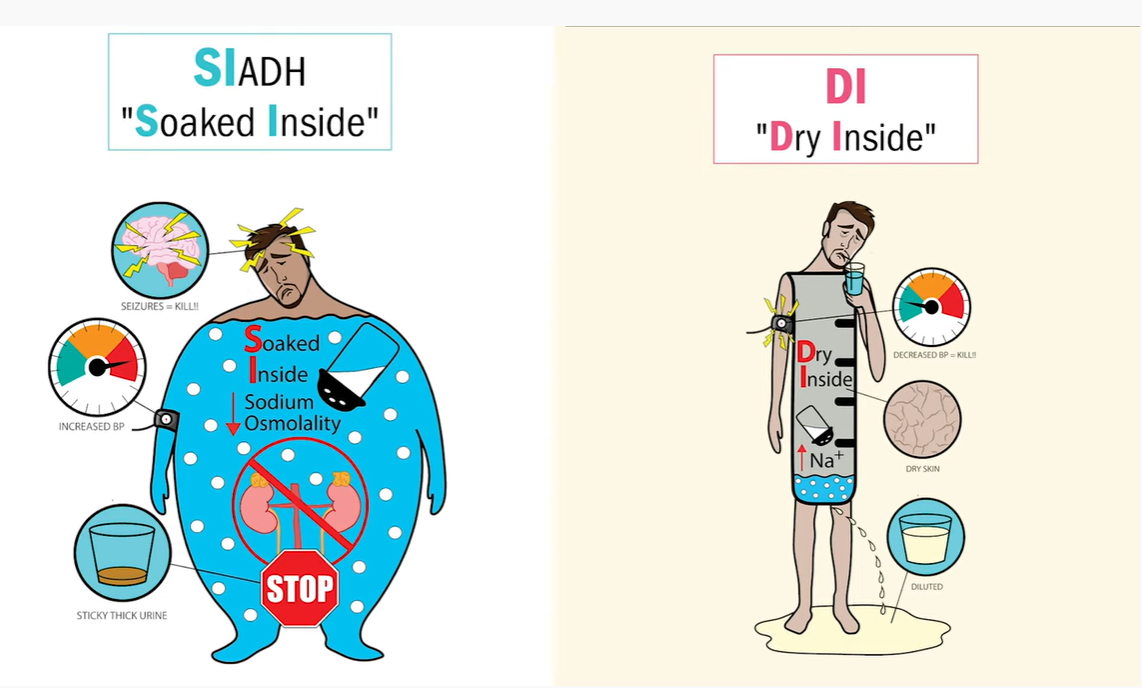
Diabetes insipidus is a disorder characterized by an inability to concentrate urine, leading to excessive urination and thirst. It results from a deficiency of antidiuretic hormone (ADH) or a lack of response to ADH by the kidneys. There are two main types:
- Central (Neurogenic) DI: Caused by a deficiency of ADH due to damage to the hypothalamus or pituitary gland from injury, infection, surgery, or tumors.
- Nephrogenic DI: Caused by the kidneys’ insensitivity to ADH, which can result from genetic disorders, chronic kidney disease, or certain medications.
Symptoms
- Polyuria: Excessive urination, often several liters per day.
- Polydipsia: Excessive thirst, leading to increased fluid intake.
- Dehydration: Dry skin, mucous membranes, and decreased skin turgor.
- Electrolyte Imbalance: Hypernatremia (high sodium levels) due to loss of free water.
Risk Factors
- Head Trauma: Injuries affecting the hypothalamus or pituitary gland.
- Genetic Factors: Inherited forms of nephrogenic DI.
- Medications: Lithium and other drugs that affect kidney function.
- Chronic Kidney Disease: Impaired kidney response to ADH.
Diagnosis
- Water Deprivation Test: Measures the body’s ability to concentrate urine when fluids are restricted.
- ADH Levels: Low levels in central DI and normal or high levels in nephrogenic DI.
- Urine Osmolality: Low urine osmolality despite high serum osmolality.
- Desmopressin Test: Response to desmopressin (synthetic ADH) differentiates between central and nephrogenic DI.
Management
- Desmopressin: Synthetic ADH used in central DI.
- Thiazide Diuretics: Reduce urine output in nephrogenic DI.
- Dietary Modifications: Low-sodium diet to reduce urine output.
- Hydration: Ensuring adequate fluid intake to prevent dehydration.
- Patient Education: Importance of medication adherence and monitoring for symptoms of dehydration and electrolyte imbalance.
Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
Pathophysiology
SIADH is a disorder characterized by excessive release of ADH, leading to water retention, dilutional hyponatremia, and concentrated urine. It results from inappropriate production of ADH due to various causes, including:
- CNS Disorders: Head trauma, infections, tumors, or stroke.
- Pulmonary Disorders: Pneumonia, tuberculosis, or positive pressure ventilation.
- Medications: Drugs that stimulate ADH release or enhance its action (e.g., antidepressants, antipsychotics, chemotherapy).
- Malignancies: Ectopic production of ADH by tumors (e.g., small cell lung carcinoma).
Symptoms
- Hyponatremia: Low sodium levels leading to nausea, vomiting, headache, and confusion.
- Water Retention: Weight gain and edema.
- Neurological Symptoms: Seizures, altered mental status, and coma in severe cases.
- Low Urine Output: Despite high fluid intake.
Risk Factors
- CNS Disorders: Conditions affecting the brain.
- Lung Disease: Pulmonary infections and chronic lung conditions.
- Cancer: Especially lung cancer and other malignancies.
- Medications: Drugs known to affect ADH secretion.
Diagnosis
- Serum Sodium: Low sodium levels (<135 mEq/L).
- Serum Osmolality: Low serum osmolality (<280 mOsm/kg).
- Urine Osmolality: High urine osmolality despite low serum osmolality.
- Urine Sodium: Elevated urine sodium concentration (>20 mEq/L).
- Exclusion of Other Causes: Rule out other conditions causing hyponatremia.
Management
- Fluid Restriction: Limiting fluid intake to prevent further dilution of serum sodium.
- Salt Tablets or Hypertonic Saline: To raise serum sodium levels in severe cases.
- Medications: Demeclocycline or vasopressin receptor antagonists (vaptans) to reduce ADH effects.
- Treat Underlying Cause: Addressing the underlying condition causing SIADH.
- Patient Education: Importance of adhering to fluid restrictions and recognizing symptoms of worsening hyponatremia.
NCLEX Preparation Tips for DI and SIADH
- Understand Pathophysiology: Be clear about how DI and SIADH occur and their underlying mechanisms.
- Memorize Key Symptoms: Recognize the classic symptoms of DI and SIADH.
- Diagnostic Tools: Familiarize yourself with the various tests used to diagnose DI and SIADH and their significance.
- Management Strategies: Know the acute and long-term management protocols for DI and SIADH.
- Complications: Be aware of potential complications and their interventions.
- Practice Questions: Utilize NCLEX practice questions focused on DI and SIADH to reinforce your knowledge and improve your test-taking skills.
Related posts